
30 tips for living well with CLL (an update of "Coping Strategies" and "Things we can do...")
30 tips for living well with CLL (an update of "Coping Strategies" and "Things we can do...")
This is a collection of practical tips gathered from this forum over the years, to help us live better with CLL. I’ve added some personal comments, saying how I myself have taken on board some of these suggestions.
Single-cell sequencing of CLL therapy: Shared genetic program, patient-specific execution
Single-cell sequencing of CLL therapy: Shared genetic program, patient-specific execution
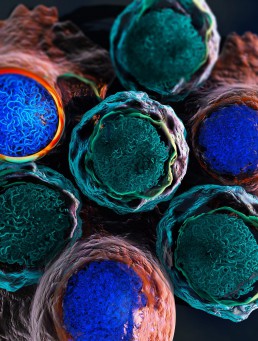
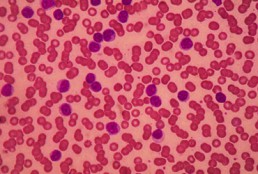
Chronic lymphocytic leukemia (CLL) is the most common form of blood cancer (leukemia) in the Western world, affecting approximately 1.2% of all cancer patients. This type of cancer starts with the lymphocytes (a type of white blood cells) that are produced in the bone marrow. CLL is characterized by the proliferation of abnormal lymphocytes (B cells) that fail to mature and grow out of control. These abnormal cells accumulate in the bone marrow and lymph nodes, taking the place of other healthy cell types and impeding their normal development. Finding the most suitable therapy for each patient poses a challenge due to the clinical and molecular heterogeneity of this disease, with some patients facing slow disease progression, whereas others face rapid progression and require quick medical response.
The cancer drug ibrutinib, a Bruton tyrosine kinase (BTK) inhibitor, has remarkable efficacy in most patients with CLL. It is becoming the standard of care for most patients requiring treatment due to its clinical efficacy and mostly tolerable side effects. However, it does not cure the disease, and patients must undergo prolonged periods of treatment. Christoph Bock and his group at CeMM investigated the molecular program with which CLL cells and other immune cells response to ibrutinib treatment in patients with CLL. Their goal was to learn the epigenetic and transcriptional patterns that predict how swiftly the treatment is having an effect on the CLL cells and how long it takes for the disease to respond in each individual patient.
More Specific BTK Inhibitor Shows High Relative Rates of Response in CLL
More Specific BTK Inhibitor Shows High Relative Rates of Response in CLL
In a phase 3 trial, acalabrutinib, a second-generation Bruton’s tyrosine kinase (BTK), provided a progression-free survival (PFS) advantage over a chemotherapy-containing standard in frontline treatment of chronic lymphocytic leukemia (CLL).
In the three-arm study, called ELEVATE TN, acalabrutinib (Calquence, AstraZeneca) alone and in combination with obinutuzumab (Gazyva, Genentech) was found to be significantly more effective than chlorambucil plus obinutuzumab for the primary PFS end point, reported investigator Jeff P. Sharman, MD, at the 2019 annual meeting of the American Society of Hematology (ASH, abstract 31). Dr. Sharman, the director of research at Willamette Valley Cancer Institute, in Eugene, Ore also noted that a trend toward an overall survival (OS) benefit appeared to be emerging for the acalabrutinib combination.
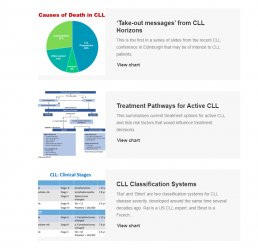
Slides from Edinburgh
Slides form Edinburgh
Why are Online Communities a Good Idea?
- A new diagnosis can be a scary, and lonely, time.
- Online communities like CLLANZ, HealthUnlocked, and Patient Power are helping people come together, and cope with complex chronic illnesses such as CLL.
- The patients’ shared experiences and knowledge of their condition, hospitals, healthcare services and drugs is leading to improvements in patient care, both by themselves, and by their carers, and their doctors.
- Knowledgeable patients become their own advocates and ask questions of their doctor, forming a partnership approach.
Chronic Lymphocytic Leukaemia
- Most common adult leukaemia
- Most patients are older than 65
- Cancer of the immune system affecting B-cells
- Can present with a weak immune system
- Each patient’s CLL is different
- Most patients will, often initially, not require treatment. Watch and wait (and worry)
- Most new therapies have improved the prognosis of CLL, but it still remains a chronic condition that can only rarely be cured
Initial Workup of CLL Patients
- All patients at diagnosis
-Flow cytometry (via blood and / or bone marrow) to confirm CLL diagnosis
- Informative for prognosis and / or therapy determination
-Del17p, and del11q. These portend for more aggressive disease
-Mutated / unmutated VH gene status assessment (not yet available in New Zealand).
-No CT scan unless symptoms are present: PET scan can be helpful if Richter’s suspected
- Bone marrow biopsy and aspirate not necessary in absence of cytopenias

Ibrutinib and Venetoclax Combo ‘Impressive’ in Front-Line CLL
Ibrutinib and Venetoclax Combo ‘Impressive’ in Front-Line CLL
The combination of two targeted therapies — ibrutinib (Imbruvika, Pharmacyclics/Janssen) and venetoclax (Venclexta, AbbVie) – has shown impressive results in the front-line treatment of chronic lymphocytic leukemia (CLL).
To read the full story visit Medscape
RIP Clive James
RIP Clive James
Clive James, the Australian wit, broadcaster and poet died last Sunday at the age of 80, ten years after being diagnosed with CLL.
He wrote the best — the only? – poem about chemotherapy, specifically about Ibrutinib. the wonder drug that helped keep him and many thousands of others alive for a lot longer than expected. Here it is:
Ibrutinib
The Marvel Comic name should tip you off
That this new drug is heavy duty stuff.
You don’t get this one just to cure a cough.
A chemo pill, and powerful enough
To put the kibosh on your CLL,
It gets in there and gives the bastard hell.
Five years’ remission and the beast is back.
It’s in your bones the way the Viet Cong
Poured through their tunnels to the Tet attack,
And what comes next might not last very long.
But let’s see what Ibrutinib can do
To win the war whose battlefield is you.
Ibrutinib, you little cluster-bomb
Of goodness, get in there and do your thing!
All that the bad guys seek is martyrdom:
Their own demise is the death they bring.
They work in cells. There is no high command.
We let you in and then it’s hand to hand.
Should you prevail, we promise you a role
From here on until the natural end.
Just beat them back and it will be a stroll,
Unless you don’t, in which case things might tend
To go bananas in a serious way.
But not yet. Down the hatch. This is today.
***
Inspirational stuff — and Ibrutinib really is a remarkable drug, a pill rather poisonous goo, showing the way to targeted treatment of leukaemias and other cancers. Only Clive James could make it sound so poetic!

Most anticipated studies on chronic lymphocytic leukemia at ASH
Most anticipated studies on chronic lymphocytic leukemia at ASH
This article was originally published on Healio
In this Guest Commentary, Ryan W. Jacobs, MD, principal investigator of clinical trials for chronic lymphocytic leukemia at Atrium Health’s Levine Cancer Institute, reviews studies on CLL that will be presented at the ASH Annual Meeting and Exposition. The most anticipated trials will reveal new information on BTK plus BCL-2 inhibition, updates on major clinical trials — including the CLL14 and MURANO trials — early data on CAR T-cell therapy, and more.
There are a lot of studies updating us on new treatment options for CLL, which is not surprising given how rapidly the field has been progressing. Essentially all the major newer drugs being used to treat CLL have some significant updates. There is also a lot to be excited about regarding where the field may be progressing to in terms of chemotherapy-free small molecule inhibitor combinations that are administered over a defined timeline, produce deep remissions and are well tolerated. This will be a review of the notable oral presentations in CLL.
BTK plus BCL-2 inhibition
There has been evidence and recognition for a while now that using both BTK and BCL-2 inhibition together makes sense in terms of complimentary mechanisms of action, the potential to reduce possible mechanisms of resistance, and how well these drugs treat disease in different sanctuaries of the body. For example, ibrutinib (Imbruvica; Pharmacyclics, Janssen), a BTK inhibitor, targets disease well in the enlarged lymph nodes and spleen. Venetoclax (Venclexta; AbbVie, Genentech) is really good at clearing out the circulating disease quite rapidly.
There are five noteworthy oral presentations evaluating the combination of BCL-2 inhibition and BTK inhibition. The most significant in terms of the number of patients on the trial and the length of follow up is the phase 2 CAPTIVATE study (Tam CS, et al. Abstract 35), which looked at the combination of ibrutinib plus venetoclax for 1 year after a 3-month lead-in with ibrutinib (I acknowledge I may be biased as I am a contributing author). The study enrolled 164 patients aged younger than 70 years, which is more than double the number of patients compared with the other oral presentations that are investigating this combination. CAPTIVATE is also unique in that it is not restricted to high-risk patients, which one of the other trials specifically focuses on. This trial looked at MRD negativity in both the peripheral blood and the bone marrow at the end of 1-year combined therapy. That is the information that is going to be reported because the median follow up is only 14.7 months so far, which is not long enough to fully analyze PFS data. The combination seems to be very effective — close to a 100% overall response rate. At the 1-year mark of combined therapy, the highest reported rates of bone marrow MRD negativity was 71%. The concordance rate between MRD negativity and peripheral blood was very high at 93%. This means that most of the patients who were MRD negative in the blood were also MRD negative in the bone marrow.

Cancer Control Agency open, Prime Minister hails Blair Vining's 'tireless advocacy'
Cancer Control Agency open, Prime Minister hails Blair Vining's 'tireless advocacy'
This story was originally published on Stuff
The Prime Minister has acknowledged Blair Vining’s “tireless advocacy” as the new independent Cancer Control Agency was formally opened on Tuesday.
During Vining’s final months, as he was dying from cancer, the Southlander pushed for the Government to set up an independent cancer agency to improve cancer care for New Zealanders.
In September, a matter of weeks before Vining died, he attended an announcement in Auckland where Prime Minister Jacinda Ardern revealed the Government’s Cancer Action Plan, which included setting up a cancer agency.
On Tuesday, weeks after Vining’s death, the cancer agency has been opened.
Ardern pointed to the work of Vining when she announced the agency as open.
“I want to acknowledge those who’ve worked so hard to ensure better cancer care in New Zealand, especially Blair Vining whose tireless advocacy for the establishment of this agency has left an important legacy,” Ardern said.
”Today’s official opening marks the start of a new era for cancer care in New Zealand. The Cancer Control Agency will play a critical role in ensuring all New Zealanders get world-class cancer care, no matter who they are or where they live.”
Ardern and Minister of Health David Clark also announced the makeup of the advisory council that will support.
Included is Dr Chris Jackson, a medical director of the Cancer Society, medical oncologist, and senior lecturer at the University of Otago.
Jackson was also Vining’s doctor and the pair became close as they battled together for better cancer care in New Zealand.
Other council members include Dr Ashley Bloomfield, Dr Nina Scott, Dr Richard Sullivan, Shelly Campbell, Graeme Norton, Professor David Tipene-Leach, and Alisa Care.
Professor Diana Sarfati has been appointed by the State Services Commission as interim chief executive for the agency.
Health Minister Dr David Clark said recruitment was underway to bring the agency up to close to 40 full time staff.
“Professor Sarfati and her team will be supported by [the] advisory council made up of leading clinicians, experts and consumer representatives. The calibre of the people who have agreed to be members of the council speaks for itself, and shows just how committed the entire health sector is to making progress on cancer.”
Consultation on the Cancer Action Plan has now been completed, with nearly 400 submissions received from individuals and organisations.
The final plan will be released early next year.
Petition for Patient Voice Aotearoa: Reform Pharmac and double the Pharmac budget
Petition for Patient Voice Aotearoa: Reform Pharmac and double the Pharmac budget
There are issues involving Pharmac and how they fund medicines – Pharmac does not adopt international guidelines; it does not set a timeframe by which it will be decided if a medicine is efficacious and another timeframe when it will endeavour to fund a medicine if it is deemed to be efficacious; it needs to establish a rapid access scheme; and the budget needs to be increased as its budget is just over 5% of the Vote Health budget in comparison with the OECD average of 16%.
Sign the petition here: https://www.parliament.nz/en/pb/petitions/document/PET_91080/petition-of-malcolm-mulholland-for-patient-voice-aotearoa
Follow Patient Voice Aotearoa here on Facebook: https://www.facebook.com/patientvoiceaotearoa/