
Understanding your connection with Clinical Trials 2021
Understanding your connection with Clinical Trials 2021
Andrew Schorr has kindly shared this on our CLL Advocates NZ Private Facebook Group which we thought was well worth sharing further.
“Some of us have been in a clinical trial? Have you? I have been in two. And if you haven’t, how come? Later this month I am the keynote speaker for 1,000 scientists and coordinators who run trials worldwide. They want to hear from me and you. Please take 4 minutes and participate in my survey (there is no sponsor other than me!). Your privacy is protected but your experience pro or con is important. Here’s the link. Thanks for helping!
Access the survey here: https://survey.alchemer.com/s3/6490816/Understanding-Your-Connection-with-Clinical-Trials-2021
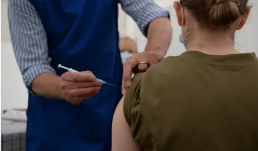
Who will be eligible for a third Covid jab in the UK?
Who will be eligible for a third Covid jab in the UK?
This article was originally published on The Guardian
Half a million people in the UK who have severely weakened immune systems are to be offered third shots of Covid vaccines in an effort to improve their protection against the disease.
So what is the advice, who is eligible, and where does this leave plans for an autumn booster programme?
What is the new advice on vaccines?
The government’s independent vaccine advisers, the Joint Committee on Vaccination and Immunisation (JCVI), has recommended a third shot of Covid vaccine for people with severely weakened immune systems. The committee estimates 400,000 to 500,000 patients aged 12 and over are eligible in the UK.

An expert hematologist/oncologist highlights
An expert hematologist/oncologist highlights
This article was originally published on OncLive
Tara Graff, DO, MS: If somebody asked me the most important things to do with a newly diagnosed patient with CLL [chronic lymphocytic leukemia], first and foremost—I can’t say this enough—it’s so important to check all the different genomic aberrations. You need to know. We’re always used to, “13q, they’ve got great disease, they’re never going to need treatment.” But that’s a knee-jerk reaction. It’s important to know that, but there are so many other molecular aberrations that we need to know about, specifically 17p, TP53, and the IGHV mutational status. We need to know that. Looking back, when I’ve picked up patients who may have been seen by another provider, those weren’t checked. We could have potentially done them a disservice in the past if we gave FCR [fludarabine, cyclophosphamide, rituximab] to a patient who had an unmutated IGHV. They have a really poor response to chemotherapy-immunotherapy, but we didn’t always know that. That wasn’t always being tested routinely.

Update on treatment of Covid-19 in CLL patients
CLLANZ Newsletter August 2021 - Update on treatment of Covid-19 in CLL patients
It is well recognised that the immune response to Covid 19 infection of individuals with CLL is markedly poorer than that of the general population, with associated increased hospitalisation rates, and increased mortality from the disease. It is thought that about 40% of patients with CLL do not develop an adequate antibody response to Covid 19 infection, or to Covid 19 vaccinations.
For this reason we can be much encouraged by the major recent therapeutic development of a monoclonal antibody to treat or reduce the risk of developing acute Covid 19 infection.
This antibody is known as Ronapreve in the UK and REGEN-COV in the US, and is a combination of two antibodies, casirivimab and imdevimab. It is produced by Regeneron Pharmaceuticals with Roche. Roche is the NZ distributor.
It can be given to at-risk patients as a single dose, IV or subcutaneously after any exposure to a Covid 19 infected individual or with the development of Covid 19 symptoms, in particular for those with a reduced/absent Covid 19 antibody response such as CLL patients. It has been shown to reduce dramatically the rates and duration of the clinical illness (80%), hospitalisation rates (70%), and mortality (25%).
Anyone with CLL who gets Covid 19 symptoms, or has close contact with someone with Covid 19 infection, should immediately self-isolate and call Healthline. But they should also ask the medical staff making their assessment about consideration of this monoclonal antibody as treatment for their condition.
Other monoclonal antibodies are also in the pipeline in relation to Covid 19, including tocilizumab, currently being considered by Pharmac for funding for cases of severe Covid 19 pneumonia.
There are additional aspects of Covid 19 infection risk-reduction that should also be part of all CLL patients’ plans/behaviour. Vaccination is of course the big one, and is central to prevention and reduction in severity of Covid 19 infection. There is mounting evidence that CLL patients should have three vaccination shots, the third being a ‘booster’, which is believed to improve the vaccine response especially in the subgroup with a low antibody response.
I’m sure you will be more than familiar with the other now routine infection-prevention measures such as wearing masks, avoiding crowds and poorly ventilated areas, regular hand washing and social distancing.
Stay safe!
With best wishes
Neil Graham

World CLL Day - 1 September
World CLL Day - 1 September
Every 1 September, the global CLL community unites to raise awareness about Chronic Lymphocytic Leukemia (CLL) and give those affected by a diagnosis of CLL a much needed voice. On World CLL Day we come together to improve understanding of the vulnerability of CLL patients and the challenges involved in living with CLL.
Access and share WCLLD21 Campaign Materials
You will find a variety of online resources for easy download to promote World CLL Day on your Social Media accounts and other online channels. You can either download specific images by clicking on the image of your choice in the overview below OR you click on the red button below to go to full set of Campaign Materials adjusted for different Social Media channels.


Responses to COVID-19 Vaccines Vary in Patients With Hematologic Malignancies
Responses to COVID-19 Vaccines Vary in Patients With Hematologic Malignancies
This article was originally published on Cancer Therapy Advisor
Patients with hematologic malignancies are known to be at risk of severe outcomes from COVID-19, and experts have recommended prioritizing these patients for COVID-19 vaccination.1,2
However, research has suggested that patients with hematologic malignancies may not mount an effective antibody response to vaccination.3
A study recently published in Cancer Cell provides insight into which hematologic malignancies and anticancer treatments confer a greater risk of poor antibody response, as well as which vaccine may be more likely to produce a response in patients with blood cancers.
To continue reading this article on Cancer Therapy Advisor
The Medicine Gap
The Medicine Gap
Many New Zealanders who try to effect change by advocating for help or medicines support from Pharmac or the Government do so at a very vulnerable time in their lives.
They, or their loved ones are often ill or trying to come to terms with a life-threatening or terminal diagnosis. Often, they are lone voices calling for change or help. Always, it is a David versus Goliath battle.
The Medicine Gap is helping to provide a collective voice to the thousands and thousands of New Zealanders who need help to stay well or to stay alive.
It is our hope that every New Zealander understands the medicines predicament we are in and will join our call to provide First World access to modern medicines for New Zealanders.
– The Medicine Gap

Upcoming CLL events
Upcoming CLL events
International Awareness
Leukaemia and Blood Cancer (LBC) NZ – Blood Cancer Forum
CLLAN Horizons Conference
5 -7 November

Pharmac commits to being more transparent
Priority lists for funding applications
On 28 July for the first time Pharmac released its ‘Options for investment list’. These are the priority medications Pharmac would like to fund if they had the budget to do so. They do not provide a ranking so we don’t know where each medication sits on the list. See the list here.

As a Cancer Patient, Will I Need an Extra Dose of a COVID-19 Vaccine?
As a Cancer Patient, Will I Need an Extra Dose of a COVID-19 Vaccine?
This article was originally posted on Patients Power
Individuals who are immunocompromised, including people with cancer, are wondering if they will need an additional dose of a COVID-19 vaccine to increase their level of protection against the coronavirus. The Advisory Committee on Immunization Practices (ACIP), which makes recommendations to the Centers for Disease Control and Prevention, met on July 22 to discuss this issue, among other topics. The meeting was a preliminary step in discussing the safety and effectiveness of additional vaccine doses before any new recommendations can be made.
When a person has cancer, there are two main reasons why they have an increased risk of infection: Either the disease itself or its treatment may cause suppression of the immune system. When this happens, a person may be considered immunocompromised. It is estimated that close to 3% of the U.S. population is immunocompromised, including those with solid tumors and blood cancers, people who have had organ or stem cell transplants, and those being treated with drugs that affect the immune system, including certain chemotherapy medications and corticosteroids.
While research indicates a very strong response to the COVID-19 vaccines in the general population, there is growing evidence that some people who are immunocompromised have a less robust immune response, even after they have been fully vaccinated.
Let’s review a bit. With rare exceptions, it is vital for everyone with cancer to get a COVID-19 vaccination as soon as they can, including those on most active treatments. Many experts at the ACIP meeting reemphasized the importance of vaccinations for people who are immunocompromised and further pointed out the key role of a “circle of protection” surrounding those who are immunocompromised consisting of other vaccinated individuals. It is important that all household members and others you are in close contact with are vaccinated.