Coutre Evaluates Treatment Options in Relapsed/Refractory CLL
Coutre Evaluates Treatment Options in Relapsed/Refractory CLL
This article was originally published by Targeted Oncology
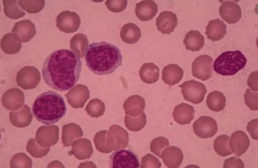
During a virtual Case Based Peer Perspectives event, Steven Coutre, MD, professor of Medicine (Hematology), Standford University Medical Center, reviewed a case of a 53-year-old woman who first presented with elevated white blood cell count. The patient was later diagnosed with chronic lymphocytic leukemia (CLL).
Targeted Oncology™: What are your initial impressions of this case?
COUTRE: I think we’d all agree that this is a patient who requires observation at this point. Clinically, this patient is at Rai stage 0. That 1 × 1 cm [lymph node] doesn’t qualify as lymphadenopathy. It certainly doesn’t need a CT scan or a bone marrow, and we can choose whether to do mutation analysis or FISH, but those results are not going to change the management approach.
To establish a diagnosis, flow cytometry was carried out showing the typical immunophenotype. Additional testing was conducted, showing the patient has no cytogenetic abnormality by FISH. Unfortunately, the patient had a bone marrow done, and it showed evidence of CLL. She was observed and did fine for 5 years, and she’s still quite young. Her WBC count has more than doubled, she’s significantly anemic, her platelet count has gone down, and the lymphadenopathy is 4 cm × 3
What are the treatment options for this patient?
The RESONATE trial [NCT01578707] evaluated patients who were previously treated for CLL and SLL [small lymphocytic leukemia] and who were randomized to receive ibrutinib [Imbruvica] at 420 mg once daily versus IV ofatumumab [Arzerra] at an initial dose of 300 mg, followed by 2000 mg for 11 doses over 24 weeks.¹
It’s no big surprise how well ibrutinib did compared with ofatumumab. The differences were highly significant. The most recent data involving 6-year follow-up published last year in Blood show that the median PFS [progression-free survival] is still not reached. These patients who entered this trial were not your average patients. The patient in our case would not have been eligible for the trial. Having a 4-year response to FCR would not [have met eligibility] for this trial. These were much worse relapsed patients, and yet here we are in 2020, and the median PFS has still not been reached with ibrutinib in this trial versus 8.11 months for the ofatumumab arm [HR, 0.133; 95% CI, 0.099-0.178].
COVID-19 Severity in CLL Correlates With 3 Disease Characteristics
COVID-19 Severity in CLL Correlates With 3 Disease Characteristics
This article was originally published by Targeted Oncology
The severity of coronavirus disease 2019 (COVID-19) increases with age in patients with chronic lymphocytic leukemia (CLL). However, age and the existence of comorbidities may not impact death from COVID-19, according to results from a retrospective international study published in Leukemia.
The study was conducted through a collaboration between the European Research Initiative on CLL (ERIC) and CLL Campus. Study results came from a survey completed by 121 investigators at 118 sites around the world. Of the survey responder, 58 investigators confirmed that there were COVID-19 cases in their CLL cohort. The majority of the cases were identified in Europe (74%), followed by Asia (13.6%), Latin America (4.2%), Africa (3.4%), Canada (2.5%), and Australia (1.7%). Altogether, 156 cases of COVID-19 in patients with CLL were reported from a pool of 15,083 patients. COVID-19 cases were symptomatic and required hospitalization in 141 patients. Preventative measures for SARS-CoV-2 were reported by all but 0.8% of the sites.
“To the best of our knowledge, we present here the largest European series of patients with CLL infected by SARS-CoV-2 and experiencing COVID-19. Among the European cases (96.8% of the total) included in this project, almost 90% originated from Italy and Spain, hence mirroring the dynamics of the SARS-CoV-2 pandemic in Europe with Italy being the first country in a number of infected individuals followed by Spain, with a lower incidence,” wrote the study authors led by Paolo Ghia, MD, PhD of the Università Vita-Salute San Raffaele.

Understanding Chronic Lymphocytic Leukemia
Understanding Chronic Lymphocytic Leukemia
This article was originally published by Cure
Episode 3
Living with CLL as a Chronic Disease
Transcript:
Kristie L. Kahl: Should patients be getting retested if or when their disease recurs?
Dr. Susan O’Brien: There are some tests that we should be repeating anytime we’re considering a new treatment, that includes the FISH test which looks at chromosomal abnormalities inside the CLL cell as well as an important protein abnormality called the p53 mutation. A p53 mutation is a gene that can be mutated and the reason it’s super important to know about these chromosomes and the p53 status is that those patients should never receive chemo or chemo-immunotherapy because they don’t respond very well to it. But even with the small molecule therapies that we have nowadays, patients with those abnormalities can do better on one drug than another. So in other words, it’s important to know that because it may affect the physician’s choice of treatment.
Kristie L. Kahl: Outside of testing, are there other factors that should be considered when it comes to determining the next line of treatment?
Dr. Susan O’Brien: When you have treatment options, which we do nowadays, you want to look at the side effect profile. If you have a patient who has a history of atrial fibrillation or an irregular heart rate…maybe in that patient you want to go towards one of the other drugs. (Venclexta [venetoclax]) can cause tumor lysis so someone with a high-volume disease maybe you would be a little bit more cautious about using that. So you want to look at the side effect profile.
The other thing that’s important is that for some of these small molecules, the length of time that the patient is on the drug is different. So what do I mean by that? With (Imbruvica [ibrutinib]) or (Calquence [acalabrutinib]), the drug is given indefinitely. So once the patient starts on it they just continue on it unless they have a side effect which makes them stop or unless x number of years later the disease starts to come back and is then resistant to the drug. With venetoclax-based therapy, the regimen that’s approved for relapse is venetoclax with the antibody (Rituxan [rituximab]) and that’s a time limited therapy. So the rituximab is given for the first six months only and then the venetoclax is given daily for two years. So that treatment actually stops at two years and that may or may not be important to the patient if they have a time-limited therapy and that may or may not be important to the patient in terms of whether continuous therapy is a problem or time limit is more attractive.
We all know that in the states with oral agents there are copays and so in some senses having a limited time duration might be attractive. On the other hand, there are some patients who say well wait a minute if I’m responding to the drug you’re going to stop it anyway and they don’t like that idea so they actually would prefer to have an indefinite therapy as long as they’re tolerating it and it’s working.
So, I think you have to look at the side effect profiles of the drugs, that they’re different durations of time and then what the patient preferences might be or what’s most important to them.
Ibrutinib May Improve CAR T-Cell Production for Patients With Chronic Lymphocytic Leukemia
Ibrutinib May Improve CAR T-Cell Production for Patients With Chronic Lymphocytic Leukemia
This article was originally published by Targeted Oncology
Ibrutinib (Imbruvica) during chimeric antigen receptor (CAR) T-cell culture improved the yield and function of CAR T-cell products as treatment of patients with chronic lymphocytic leukemia (CLL) in a study published in the International Journal of Cancer.
The study investigators led by Leapold Sellner, MD wrote, “our study provides evidence that BTK/ITK inhibition with ibrutinib during CAR T-cell generation may improve CLL patient-derived CAR T cell products and may have the potential to enhance CAR T-cell function. Ibrutinib-supplemented CAR T-cell production leads to increased CAR T-cell yields as well as enriches for less-differentiated T cells with lower expression of exhaustion markers and could be an option to further improve the clinical outcome of CLL patients.”
Sellner et al evaluated the absolute cell numbers during CAR T-cell generation by Trypan blue staining. During cell generation, cell proliferation was significantly lower in CLL-derived cells compared with HD-derived cells. The BTK inhibitor allowed for a significant increase in cell expansion of HD-derived cells on day 10 of the CAR T-cell generation (20.67 ± 8.82 × 106 without ibrutinib vs. 25.28 ± 10.29 × 106 with ibrutinib; P =.0248), and ibrutinib appeared to significantly increase the viability of CD3-positive T cells from HDs on day 10 (3% ±8% vs 87% ± 7%; P =.0183) and day 14 (84% ± 8% vs 91% ± 6%, respectively; P =.0202).
TML Helps Predict Time to Treatment in CLL and its Precursor, Study Shows
TML Helps Predict Time to Treatment in CLL and its Precursor, Study Shows
This article was originally published by AJMC
Tumor mutational load (TML) can be used as a prognostic indicator in patients with chronic lymphocytic leukemia (CLL) and high-count monoclonal B-cell lymphocytosis (HC MBL), according to a new study.
The findings suggest that performing a focused mutation panel on recurrently mutated CLL genes could help risk-stratify patients and more accurately predict time to treatment (TTT).
Most patients who are newly diagnosed with CLL do not require therapy for a number of years, but some patients will require therapy right away. CLL’s precursor, HC MBL, will progress to CLL at a rate of 1-5% per year, but it can be difficult to predict how soon an individual patient will progress.
In hopes of better predicting patient progression, investigators from the Mayo Clinic conducted a study to analyze the total number of recurrently mutated CLL genes (TML) and the individually mutated genes beyond the CLL international prognostic index (CLL-IPI) in newly diagnosed patients with CLL and HC MBL.
To do so, they recruited 557 patients, 445 of whom had CLL and the remainder of whom had HC MBL, and sequenced 59 genes in the patients. Their goal was to identify links with TTT, adjusted for CLL and sex.
The authors found that TML correlated with shorter TTT. Among patients with low/intermediate risk, the link was even stronger when patients were stratified by CLL-IPI. Their results are published in the American Journal of Hematology.
Ball Score Predicts Benefit From Ibrutinib in CLL
Ball Score Predicts Benefit From Ibrutinib in CLL
This article was originally published by MedScape
The BALL score was able to identify a subset of patients with chronic lymphocytic leukemia (CLL) who particularly benefit from single-agent ibrutinib therapy, according to the results of a study of 111 patients followed from two different institutions.
The BALL model consists of four factors: serum beta₂-microglobulin at 5 mg/dL or greater, hemoglobin < 110 g/L for women or < 120 g/L for men, lactate dehydrogenase [LDH] > upper limit of normal [UNL], and time elapsed from last therapy less than 24 months. Each parameter was alloted 1 point, leading to a stratification of patients into three different prognostic groups: low risk (score 0-1), intermediate risk (2-3), and high risk (score 4), according to a report published online in Leukemia Research.
According to Stefano Molica, MD, of the Azienda Ospedaliera Pugliese-Ciaccio, Catanzaro, Italy, and his colleagues, the majority of patients (82%) were clinical Rai stage II-IV. The median patient age was 63 years and nearly 68% were men.
The researchers assessed four models for predicting overall survival. The modified version of CLL-International Prognostic Index (CLL-IPI) failed to provide prognostic information in relapsed/refractory (R/R) CLL (P = .77) as did the Ahn et al. model (P = .95) and a simplified BALL model (P = .09). In contrast, the full BALL score captured two groups of patients with significant differences in survival (hazard ratio, 0.240; 95 % confidence interval, 0.10-0.54; P = .0005); however, because of the low number of patients in the high-risk category, these cases were combined with the intermediate-risk group.
The BALL score identified a subset of patients, accounting for about 50% of the whole population, who particularly benefit from single-agent ibrutinib, according to Dr. Molica and his colleagues. These patients had a survival rate of 85% at 3 years.
“In contrast, the outcome of subjects with intermediate-high risk is disappointing. These patients should be considered for a combination of targeted drugs or cellular-based therapies,” the researchers concluded.
Cohen Expands on Treatment Options in Patients With Genomic Aberrations in CLL
Cohen Expands on Treatment Options in Patients With Genomic Aberrations in CLL
This article was originally published by Targeted Oncology
During a virtual Case Based Peer Perspective event, Jonathon B. Cohen, MD, MS, the codirector of the Lymphoma Program, medical director of Infusion Servies, and associate professor in the Department of Hematology and Medical Oncology at Emory University School of Medicine and Winship Cancer Institute, discussed a case of a 71-year-old woman diagnosed with chronic lymphocytic leukemia.
Targeted Oncology™: What are reasonable treatment options to consider in a patient with CLL?
COHEN: The National Comprehensive Cancer Network guidelines offer 6 treatment options for patients with del(17p).1 As I tell my fellows when I work with them, if you ever see a list of preferred regimens with 6 options, that likely means that nobody really knows what the best option is.
The 1 option not listed in the guideline is chemotherapy, especially in the relapsed setting for patients with del(17p). I generally would not use chemotherapy.
The only exception to that might be a situation where we have a patient who’s young and for whom we’re thinking about moving on to something like an allogeneic transplant or some other definitive therapy. We might consider using chemotherapy for a cycle or 2. But otherwise, if you’re not going in that direction, that’s the 1 thing we do feel comfortable saying—that is, that chemotherapy is probably not the right option.

FDA Clears clonoSEQ to Detect MRD in Chronic Lymphocytic Leukemia
FDA Clears clonoSEQ to Detect MRD in Chronic Lymphocytic Leukemia
This article was originally published by AJMC
Adaptive Biotechnologies received its third approval from the FDA for the use of its next-generation sequencing assay to detect minimal residual disease (MRD) in chronic lymphocytic leukemia (CLL).
The assay, clonoSEQ, uses a proprietary immunosequencing platform to monitor for MRD, where a small number of cancer cells remain during and after treatment. It is difficult to detect without precise, sensitive tools, and can lead to a recurrence of disease.
The approval follows a decision by CMS in January to pay for cloneSEQ testing for CLL, in addition to multiple myeloma and B-cell acute lymphoblastic leukemia. Nearly 80% of US patients with CLL are age 65 or over.
Continue reading this article on AJMC
Experts Outline Best Practices in the Treatment of Chronic Lymphocytic Leukemia
Experts Outline Best Practices in the Treatment of Chronic Lymphocytic Leukemia
This article was originally published by Pharmacy Times
Chronic lymphocytic leukemia (CLL) is a cancer of the blood and bone marrow that can be treated to extend the life of some patients even by decades. Treatments and best practices are developing rapidly and health care providers need to stay up to date on all relevant information. In a Pharmacy Times Insights video series, a panel of experts discussed how to best treat and monitor patients living with CLL.
The panel included Alison Duffy, PharmD, BCOP, an associate professor and clinical pharmacy specialist in oncology at the University of Maryland School of Pharmacy and Cody Steeves, PharmD, BCOP, a clinical pharmacist for Biologics by McKesson.
Both intravenous (IV) and oral CLL medications are available, each with their own benefits and disadvantages. A combination method is also used by many patients, but that also presents a unique set of challenges.
“Some of the economic challenges we’ve seen have been the timely approval of the oral and the IV therapy together because of pharmacy benefits and medical benefits, and so that can be a challenge, especially if a patient’s disease is very aggressive. If they have progressed on ibrutinib it would be really important to start their subsequent therapy very quickly, or it can progress to Richter transformation,” Duffy said. “The economic challenges in improving can be a barrier. As pharmacists, anything we can do to facilitate the approval process, and in the clinic, I can certainly help with the prior authorization process.”
Experts Discuss Treatment Advances for Chronic Lymphocytic Leukemia
Experts Discuss Treatment Advances for Chronic Lymphocytic Leukemia
This article was originally published by Pharmacy Times
In the Pharmacy Times ® Directions in Oncology™ Insights series on chronic lymphocytic leukemia (CLL), experts Alison Duffy, PharmD, BCOP, and Cody Steeves, PharmD, BCOP, discussed current treatment recommendations and what is next for the disease state.
CLL is a rare cancer of the blood and bone marrow, and although it is difficult to treat many advances have been made in the past 6 years, said Duffy, an associate professor, clinical pharmacy specialty in oncology at the University of Maryland School of Pharmacy.
Earlier recommendations included single-agent chemotherapy or single-agent monoclonal antibodies, but Duffy explained that patients are increasingly receiving small molecule inhibitors, including Bruton tyrosine kinase (BTK) inhibitors.
Without the use of single-agent chemotherapies or single-agent monoclonal antibodies, Duffy said pharmacists can see patients with CLL in many settings.
“Using those as single agents, or more commonly in combination, that’s where the pipeline and future directions are really moving towards, with combination therapy as well as more potent, more selective, targeted therapies,” she said.
According to recommendations from the National Comprehensive Cancer Center (NCCN), Duffy said some current frontline treatment agents include ibrutinib, venetoclax plus obinutuzumab, acalabrutinib with or without obinutuzumab, and chemo-immunotherapy, when warranted.
Frontline therapies present various challenges, although Duffy said the treatment criteria has become less rigid.
“Some of the things that I would think about would be age, fitness, comorbidities such as atrial fibrillation, and renal function if I was going to give something like fludarabine within the FCR [fludarabine, cyclophosphamide, and rituximab] regimen,” Duffy said.
She added that considering patient preferences and clinical experiences is important. Some patients may not be great candidates for oral therapy due to a lack of access, finance, comfort level, or adherence challenges. Similarly, transportation might be an issue for patients receiving intravenous chemotherapy and should be considered.
“Moving forward, it’s positive to see that the outcomes, when they’re stratified by those patients with the deletions, still tend to trend in the positive direction for those patients with these newer oral therapies we’ve had over the past 5 or 6 years,” Steeves said.
The experts also turned their attention to minimum residual disease (MRD) testing and how it affects the use of limited duration therapy. MRD testing is particularly helpful for diseases that require stronger treatments, Steeves said. He explained that some data has found that obtaining a low or negative MRD corresponds with significantly increased progression-free survival compared with medium or high levels of MRD. However, patients receiving oral agents, especially single-agent BTK inhibition alone or with a CD20 inhibitor, are not expected to achieve MRD. Despite the lack of MRD, Steeves said these agents can be valuable.
“Even though we’re not seeing those deep remissions with MRD negativity, undetectable MRD, we certainly are still seeing a large benefit of using these agents without that,” Steeves said.
Steeves, clinical oncology pharmacist, Biologics by McKesson, also emphasized the importance of a patient-specific treatment plan. Some patients may want to take the drug for as short a period as possible, while others find that it does not disrupt their daily lives to a large extent because they are already receiving multiple medications.
Finally, Duffy and Steeves turned their attention to BTK inhibitor monotherapy for patients with newly diagnosed CLL. Ibrutinib, a new BTK inhibitor, was investigated in the RESONATE trial (NCT01578707), which found long-term benefit of the drug upon 6-year follow-up. The trial also established ibrutinib as the first-line choice for older patients and those without a 17P deletion, thereby demonstrating significant progression-free survival benefit among those high-risk subgroups. However, Duffy noted that ibrutinib is not for everybody.
“If you have a patient with uncontrolled atrial fibrillation, who has a high risk of bleeding that can’t be mitigated, or uncontrolled hypertension despite optimizing therapy management, ibrutinib wouldn’t be my first choice,” Duffy said.
Although the various treatments all need to be evaluated based on unique patient needs, the recent developments for the treatment of CLL are very promising and exciting, Duffy concluded.
“We’re getting to have a better understanding of CLL biology and some of the prognostic indicators,” Duffy said. “These new therapies allow for treatment without some of the traditional chemotherapy agents.”
THE PHARMACY TIMES® DIRECTIONS IN ONCOLOGY™ INSIGHTS SERIES ON CLL CAN BE VIEWED AT WWW.PHARMACYTIMES.COM/INSIGHTS.