'Take-messages' from CLL Horizons
This is the first in a series of slides from the recent CLL conference in Edinburgh that may be of interest to CLL patients.
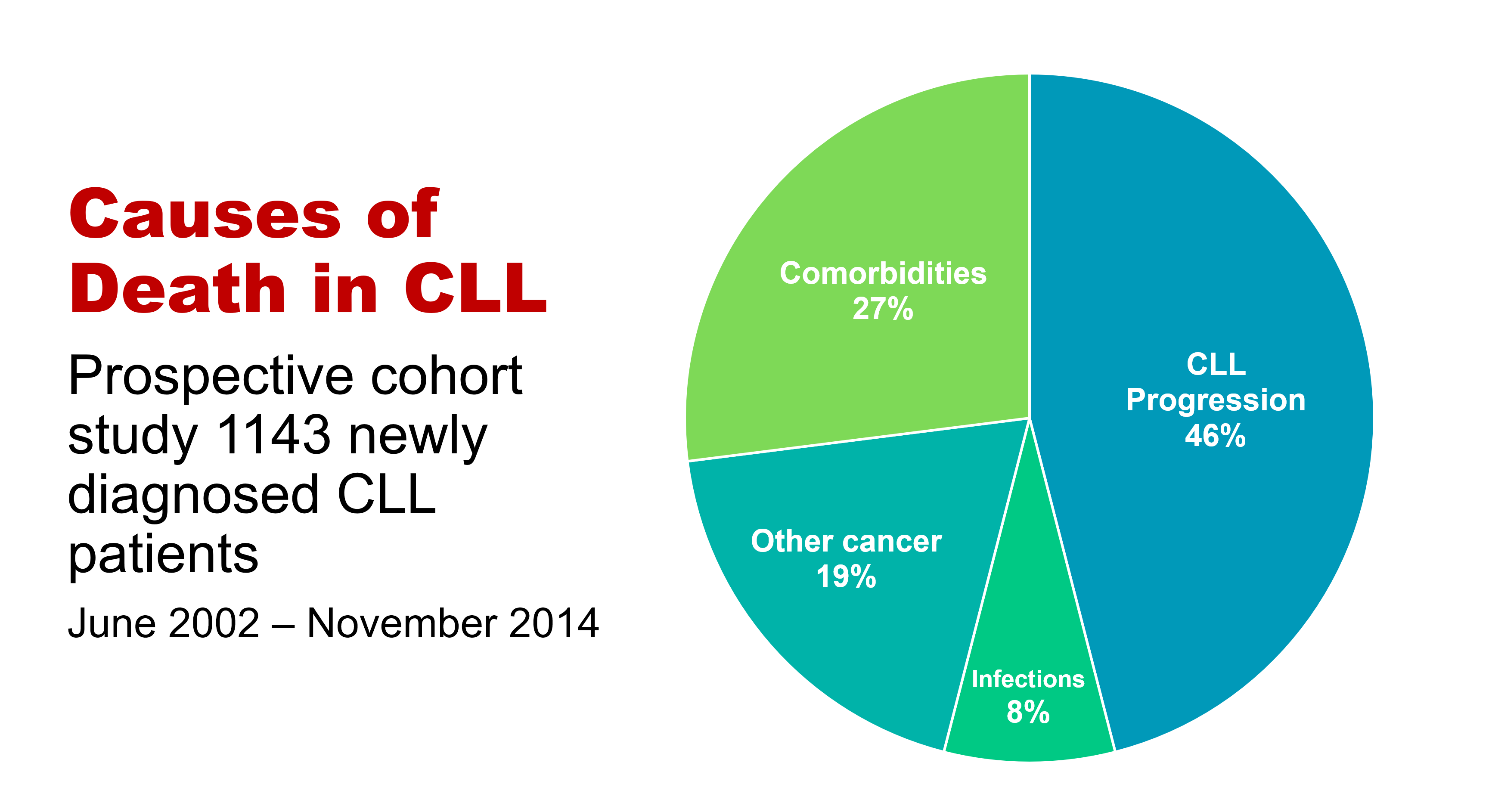
The important information here is that under half of people with CLL die primarily of that disease, while the rest die of other cancers, infections, or other diseases (comorbidities). So, if you have CLL, it’s important to be checked regularly for other cancers, such as melanoma and other skin cancers, prostate cancer in men, breast cancer in women, and gastrointestinal (oesophageal, stomach, and colon) cancers and lung cancer, in both sexes. This relates to the fact that people with CLL have a reduced ability to control cancer in their bodies because of the impaired immune system that goes with the disease.
If you develop any infection, take it seriously, as if you have CLL you’re at higher risk of a serious episode of infectious disease or a fatal outcome, again because your immune system function is impaired. You may also need more prolonged antibiotic courses, with infective diseases in the context of CLL.
The third group of non-CLL causes of death in CLL, more than a quarter of cases, relates to pre-existing conditions such as heart disease, diabetes, and chronic obstructive pulmonary disease, which either precede or develop during the course of CLL, often independently. This is partly because approximately half of people with CLL are 70+ years old at diagnosis, and partly because a lot of people with CLL, particularly the elderly patients, have a smouldering, relatively stable or only slowly progressive form of the disease. It also makes the point that important comorbidities need to be managed optimally in people with CLL.
Neil Graham