
NICE recommends new chemo-free chronic lymphocytic leukaemia treatment
NICE recommends new chemo-free chronic lymphocytic leukaemia treatment
This article was originally published on EPR
The UK’s National Institute for Health and Care Excellence has recommended a new chemotherapy-free treatment for people with untreated chronic lymphocytic leukaemia (CLL). The institute said its recommendation of venetoclax plus obinutuzumab could benefit more than 1,000 people each year.
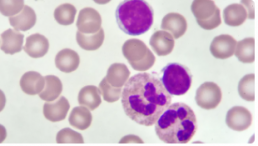
The innovative 12-month treatment will be offered to people with CLL who have not received any prior treatments. CLL affects white blood cells and is the most common chronic leukaemia, accounting for 30 percent of all adult leukaemias. In England there were 3,157 new cases of CLL in 2017.
Venetoclax plus obinutuzumab will be offered as a first-line treatment to people with CLL, with certain genetic abnormalities (such as a 17p deletion or TP53 mutation). For those without a 17p deletion or TP53 mutation, venetoclax plus obinutuzumab will be offered to patients with untreated CLL for whom fludarabine plus cyclophosphamide and rituximab (FCR) or bendamustine plus rituximab (BR) is unsuitable. The combination has also been made available via the UK’s Cancer Drugs Fund for this indication, so more evidence can be gathered on its cost effectiveness.
When and How CLL, SLL Should Be Treated
When and How CLL, SLL Should Be Treated
This article was originally published on Cure
Treatments for chronic lymphocytic leukemia (CLL) and small lymphocytic leukemia (SLL) have drastically improved in recent years, although patients may not need immediate treatment directly after being diagnosed.
Then, once it is decided that a patient will undergo treatment, deciding on the timing and regimen is pivotal.
When to Treat CLL/SLL
To determine if treatment is needed, patients should talk with their providers about symptoms they are experiencing, swollen lymph nodes, and blood cell counts, according to Dr. Locke J. Bryan, associate professor of medicine at the Medical College of Georgia and the hematology/oncology fellowship program director at the Georgia Cancer Center at Augusta University.
Bryan discussed CLL and SLL at the CURE® Educated Patient Leukemia & Lymphoma Summit.
One symptom of CLL and SLL is swollen lymph nodes; the location of the swelling could play a role in whether or not the disease is treated.
“It’s about location … a big node may not be causing any problems, but a smaller node pushing on an organ may cause some problems. Then, yes, the patient may need some treatment,” Bryan said. “And then as those (white blood cell) counts start to drop, that may be another reason.”

Dr. Awan on the Importance of Collaborative Care in CLL
Dr. Awan on the Importance of Collaborative Care in CLL
This article was originally published on Onc Live
The field of CLL continues to excel forward with novel molecular biomarkers, new therapeutic options, and ongoing clinical trials, says Awan.
Despite this, CLL remains a complex disease, Awan adds. As such, closely collaboration between community oncologists and CLL experts is often necessary to ensure patients receive optimal care.
Moreover, individuals who treat many cases of CLL may be able to recommend ongoing clinical trials that community oncologists are not aware of, Awan adds.
Ultimately, collaborative care is needed to identify new treatments and testing options, and to improve upon available therapies, Awan concludes.
Different Therapies and Modalities for Treatment of CLL in the Second Line
Different Therapies and Modalities for Treatment of CLL in the Second Line
This article was originally published on Targeted Oncology
During a Targeted Oncology Case Based Peer Perspectives event, Danielle Brander, MD, assistant professor of Medicine at Duke Cancer Institute in Durham, NC, discussed options for treating a 53-year-old female patients with chronic lymphocytic leukemia (CLL).
Targeted Oncology™: What are the guideline-recommended regimens to treat a patient with CLL such as this one?
BRANDER: The [National Comprehensive Cancer Network] guidelines for regimens in the relapsed/refractory setting include acalabrutinib [Calquence] and venetoclax [Venclexta], which are approved in all lines of therapy. In the relapsed/refractory setting, there’s also approval of duvelisib [Copiktra] and idelalisib [Zydelig], which are PI3K inhibitors.1
What data support the use of ibrutinib (Imbruvica), which is another guideline-recommended agent for the treatment of this patient?
The data that led to the initial approval of ibrutinib was the RESONATE trial [NCT01578707]. [The trial] randomized patients 1:1 to either ibrutinib or the anti-CD20 antibody standard-of-care agent in the relapsed/refractory setting, ofatumumab. Patients were allowed to cross over on this study.2
There are now 6-year follow-up data [showing that the] median progression-free survival [PFS] for the ibrutinib arm was not reached but was short [8.1 months] for the ofatumumab alone [HR, 0.133; 95% CI, 0.099-0.178].
Markers [of prognosis] that would indicate inferior response to chemoimmunotherapy are either the patients with IGHV unmutated or del(17p) or del(11q), who are still having good responses. This is in the relapsed/refractory setting with novel agents.
The grade 3 or greater AEs [adverse effects] that you’ll see are infectious complications. Infections and neutropenia do get better in terms of incidence with [time]. But obviously, if they have to stop [treatment] in the first year, it’s still detrimental to them. One thing [to keep in mind when] monitoring patients is that time on therapy does increase risks for hypertension. Atrial fibrillation and bleeding remain a risk throughout treatment. Often, they first appear early on treatment.

CLL Advocates NZ Newsletter Issue 5
CLL Advocates NZ Newsletter Issue 5
Friends of CLL Advocates NZ
I’m pleased to report on a very successful inaugural CLLANZ seminar on 14 October, co-hosted by LBC. Around 100 people attended either by zoom or in person in LBC offices up and down the country. There were three excellent presentations by three of NZ’s most authoritative clinicians on CLL. Dr Peter Browett described the disease, Dr Gillian Corbett spoke on therapy, and Dr Rob Weinkove explained likely future directions for CLL treatment. An informative panel discussion and questions session concluded the two-hour event.
I thank all those who helped organise and manage this event, and particularly LBC for providing their facilities. This will hopefully be the first of many such events in years to come.
The seminar has provided us with an up-to-date, comprehensive patient resource on CLL in NZ. A video of the full event will shortly be posted on our website, and the presentations can be found here.
Identifying the priorities we should be pushing for in CLL treatment was a key theme of the event. These included having testing available in NZ for IgVH mutations, and I’m pleased to say this has already stimulated momentum to develop this.
As well as being our inaugural seminar the event was the formal launch of CLLANZ, almost two years after we first discussed the idea of starting the group, somewhat delayed by COVID 19.
It was also the formal launch of our booklet “CLL – A Guide for Patients in NZ”. Again, dedicated individual and team effort resulted in an excellent, informative document, which is available here on our website and in hard copy. If you would like a hard copy please send us your postal address. The booklet is also being distributed to CLL clinics around NZ, where you can also pick up a copy. Feedback on this is welcomed.
We’ve already had a lot of positive feedback on the event, along with suggestions for future seminar themes, and would welcome further thoughts on this.
Best wishes
Neil Graham

Novel Prognostic Model Predictive of Survival in Ibrutinib-Treated CLL
Novel Prognostic Model Predictive of Survival in Ibrutinib-Treated Chronic Lymphocytic Leukemia
This article was originally published by Hematology Advisor
A 4-factor prognostic model may help to identify patients with chronic lymphocytic leukemia (CLL) at risk of ibrutinib failure, according to research published in the Journal of Clinical Oncology.
As CLL is a “clonal expansion of mature B cells drive by constitutive activation of B-cell receptor (BCR) signaling,” previous studies suggest that the selective inhibition of BCR and BCL-2 protein may significantly improve outcomes in some patients with CLL compared with chemotherapy as a first-line therapy.
Ibrutinib, a Bruton tyrosine kinase inhibitor, is frequently used in the CLL setting, though drug resistance invariably evolves, with relapse occurring often with ibrutinib monotherapy.
Identifying those at risk of relapse after ibrutinib therapy would improve treatment decision-making among patients with CLL. While there are existing prognostic indices, none specifically evaluate for criteria known to be linked with the evolution of ibrutinib resistance. In the present study, the researchers evaluated and validated the effectiveness of a 4-factor prognostic model among patients with CLL treated with ibrutinib.
CLL Advocates NZ Launches a New Zealand Patient Guide
CLL Advocates NZ Launches a New Zealand Patient Guide
CLL Advocates NZ is pleased to announce the official launch of its patient booklet, CLL – A Guide for Patients in New Zealand. It has been made available in both a digital download and as a hardcopy booklet.
The booklet is being launched at CLL Advocates NZ’s inaugural patient seminar in Auckland and online tonight (14 October). The seminar will discuss ‘What is the state-of-the-art treatment for CLL in New Zealand?’
The booklet was compiled by Leukaemia Care, a national UK blood cancer support charity. Leukaemia Care has kindly granted us permission to adapt the booklet for the New Zealand CLL setting, and to publish it here on our website, and make it available as a printed booklet for distribution in New Zealand. This agreement is in line with CLL Advocates NZ’s commitment to working closely with other CLL patient advocacy groups and to avoid duplicating available high quality work undertaken by others.
Adaptation of the booklet for New Zealand conditions has been undertaken by Gillian Corbett MBChB, FRACPath, MRCP, FRACP, haematologist and Trustee, CLL Advocates NZ, Neil Graham FRACP, FRCP, Executive Director, CLL Advocates NZ, and Catherine Isaac, Trustee, CLL Advocates NZ.
We are most grateful to Leukaemia Care for this very valuable contribution to our work.
To learn more about the booklet, download it, or to request a hardcopy click here.

Dr. Davids on Factors to Inform Treatment Selection in CLL
Dr. Davids on Factors to Inform Treatment Selection in CLL
This article was originally published by OncLive
Matthew S. Davids, MD, MMSc, director of clinical research in the Lymphoma Program and a medical oncologist with Dana-Farber Cancer Institute, as well as an assistant professor of medicine at Harvard Medical School, discusses factors to consider when selecting treatment for patients with chronic lymphocytic leukemia (CLL).
When deciding which modality to select for patients with CLL, comorbidities must be considered, says Davids. For example, if there is a patient with significant cardiovascular disease, particularly if he/she is on an anticoagulation medication for atrial fibrillation, BTK inhibitors may not be the optimal choice. For this patient, a venetoclax (Venclexta)-based regimen should be considered, according to Davids.
On the other hand, if a patient has poor renal function and tumor lysis risk is a concern or if he/she is older and has difficulty commuting to the medical center for frequent monitoring, then a BTK inhibitor is favored, says Davids. With this approach, there is less risk of tumor lysis and patients require less monitoring than they would with a venetoclax-based regimen, concludes Davids.
The Role of Chemoimmunotherapy Dwindles Among New Regimens in Frontline CLL
The Role of Chemoimmunotherapy Dwindles Among New Regimens in Frontline CLL
This article was originally published by OncLive
Although frontline chemoimmunotherapy regimens have been the gold standard for patients with chronic lymphocytic leukemia (CLL) for many years, the advent of BTK inhibitors and other novel drugs has moved the field toward adopting chemotherapy-free options for patients in this setting.
“For 50 years or so, there weren’t too many major developments in this field,” said Matthew S. Davids, MD, MMSc, director of clinical research and the lymphoma program at Dana-Farber Cancer Institute. “We had some improvements in the intensity of chemoimmunotherapy regimens, but in the last 10 years, we have had some really remarkable developments where the whole field was transformed.”
In an virtual presentation during the 2nd Annual Precision Medicine Symposium, a program developed by Physicians’ Education Resource® LLC, Davids, who is also an associate professor of medicine at Harvard Medical School, discussed the switch to chemotherapy-free regimens and whether chemoimmunotherapy combinations will retain a role in the frontline treatment of patients with CLL.
Novel Therapies Challenge Standard Frontline Chemoimmunotherapy Regimens
Upfront fludarabine, cyclophosphamide, and rituximab (Rituxan; FCR) chemoimmunotherapy was considered the gold standard for patients with CLL. Moreover, studies such as the FCR 300 and CLL8 trials showed that time-limited FCR can provide functional cure in patients with IGHV-mutant CLL.1,2
“This does highlight the important role of IGHV mutation status when we are thinking about using chemoimmunotherapy,” explained Davids. “IGHV-unmutated patients tend to have steady disease progression over time and do not enjoy the potential functional cure [that IGHV-mutated patients may derive].”
Other chemoimmunotherapy regimens such as bendamustine and rituximab (BR), which is widely used in the community setting, according to Davids, and obinutuzumab (Gazyva) plus chlorambucil, are also active in the frontline CLL space.
However, in recent years, studies have demonstrated superiority with novel regimens compared with chemoimmunotherapy.
“Much of [the advancements made in CLL] are due to the investment in basic science that was done in the late 1990s and early 2000s that allowed us to understand the role of the microenvironment in CLL and how that can be leveraged to treat the disease,” said Davids.
For example, in the phase 3 ECOG 1912 trial, the combination of the BTK inhibitor ibrutinib (Imbruvica) and rituximab, followed by ibrutinib maintenance therapy, demonstrated favorable progression-free survival (PFS) compared with FCR chemoimmunotherapy in patients 70 years or younger with previously untreated CLL.3
At a median follow-up of 33.6 months, the PFS rate was 89.4% with the ibrutinib/rituximab regimen versus 72.9% with chemoimmunotherapy (HR, 0.35; 95% CI, 0.22-0.56; P < .001). Moreover, overall survival (OS) also favored the chemotherapy-free regimen at 98.8% versus 91.5% with chemoimmunotherapy (HR, 0.17; 95% CI, 0.05-0.54; P < .001).
However, at 3 years, the PFS rate in patients with IGHV-mutant disease was 87.7% with ibrutinib/rituximab versus 88% with FCR (HR, 0.44; 95% CI, 0.14-1.36).
Although these chemotherapy-free options have been revolutionary in the frontline treatment of patients with CLL, chemoimmunotherapy may still be considered in this particular subgroup of IGHV-mutant patients, according to Davids.
“For my young fit patients with IGHV-mutant disease, FCR is certainly still part of the conversation,” Davids explained, adding that data suggest BR and obinutuzumab/chlorambucil are also options for these patients. In particular, BR should be considered for older, frail, IGHV-mutant patients who have cardiovascular comorbidities since giving BTK inhibitor therapy could increase the risk of cardiovascular events.
Similarly, results from the randomized phase 3 ELEVATE-TN trial demonstrated that acalabrutinib (Calquence) with or without obinutuzumab significantly improved PFS over obinutuzumab/chlorambucil chemoimmunotherapy.4 The median PFS at 28.3 months of follow-up was not reached with acalabrutinib as monotherapy or in combination with obinutuzumab versus 22.6 months with chemoimmunotherapy (HR, 0.1; 95% CI, 0.06-0.17; P < .0001; HR 0.20; 95% CI, 0.13-0.30; P < .0001).
Moreover, Davids added, chemoimmunotherapy may be selected in patients who prefer a time-limited therapy versus continuous treatment with a newer regimen.
“We can give 6 months of FCR and know that we have a good chance of very long-term remission,” said Davids. “We do have to counsel patients about cytopenias, infection risk, and secondary myeloid neoplasms. [These] are slightly more common in patients with CLL treated with FCR, but the rates are low.”
CLL14 Trial Aims to Eliminate the Need for Chemotherapy Altogether
The extended follow-up from the phase 3 CLL14 trial showed that the estimated 24-month PFS rate was 88.2% with the combination of venetoclax (Venclexta) and obinutuzumab versus 64.1% with obinutuzumab/chlorambucil.5 Although there was no statistically significant difference in OS between arms, venetoclax/obinutuzumab was associated with a low incidence of high-grade adverse effects in patients with relevant comorbidities.
CLL Advocates NZ Newsletter Issue 4
CLL Advocates NZ Newsletter Issue 4
Friends of CLL Advocates NZ
This month is Blood Cancer Awareness Month, so it was a good opportunity to reflect on collaboration, networking, and resource sharing between CLL Advocates New Zealand and other blood cancer patient support groups, which like us, are working to better understand and treat these disorders, and support those with them.
A recent and significant example of this is a current, and near complete, project of launching our ‘CLL Guide for Patients’ booklet. We have worked with and drawn upon the resources of Leukaemia Care, a national UK blood cancer support charity, to adapt their patient booklet for a New Zealand CLL setting. Within the next month CLLANZ will be launching this CLL patient guide. Leukaemia and Blood Cancer NZ (LBC) will also be launching an updated version of their own CLL booklet.
Education and learning are a major part of the way forward in your CLL journey, so I encourage you to access a copy of our booklet, which will be available in both hard copy and as a PDF download on our website. I’m sure you will find it an informative resource.
A lot of work has gone into the CLLANZ booklet, and I would like to thank Dr Gillian Corbett, Catherine Isaac, and Heather Phillips for their great work in putting the document together.
Following on from education and learning, the CLLANZ inaugural patient seminar is this coming month. Three of NZ’s experts on CLL will speak, followed by a panel discussion and questions. This is a joint event with LBC, at the LBC headquarters in Auckland, or on Zoom from anywhere, to be held on Wednesday 14 October. Registration and details can be found on our website here.
In support of other CLL patient support groups, I want to remind you of the resources and networking available globally including groups such as PatientPower and HealthUnlocked. These websites have a lot of useful information and their patient networks, while in a global setting, are very active. You can join the HealthUnlocked global community here, which boasts just under 16,000 members, and access the PatientPower CLL online events here.
There are also regular teleconferences, and other educational activities, which we have now started listing on our website here in a new events section. Many of these events are international webinars held at difficult times of the day for most of us here in New Zealand. So, we are working to access recordings of these to share with you to watch on-demand.
Another CLL group was also recently formed – Doctors with CLL, which I have joined. I will keep you posted on developments here. The umbrella organisation is CLLAN (CLL Advocates Network), based in Europe, and the organisers of the conference I attended in Edinburgh a year ago. CLLAN coordinates the activities of these groups, and there is a lot of information on their website.
There are a number of other activities also underway that I have shared recently, and which you hopefully you have in your diaries:
- Survey on participation in drug trials.
- Dr Karen Oldfield’s PhD research project questionnaire on medical marijuana use in NZ.
- Shared experiences within our group, of second malignancies that they have had in addition to their CLL.
Thank you to all of you who have been posting and engaging with material on our Private Facebook Group. Engagement from patients and supporters helps others feel confident about sharing their own stories, struggles and questions, so I encourage you to please use this platform to share resources, ask questions and comment and engage with one another. This activity will go on to help us grow the group.
Finally, the general election is this coming month. An important issue for CLL patients is funding of medications. I encourage you to look at the health policies of the significant parties and put attention on their position on Pharmac funding. A good website to look at all parties and their policies all at once is www.policy.nz. You can link directly to the health funding policies here.
Best wishes
Neil Graham