
Dr. Davids on the Potential Utility of Frontline Ibrutinib/Umbralisib in CLL and MCL
Dr. Davids on the Potential Utility of Frontline Ibrutinib/Umbralisib in CLL and MCL

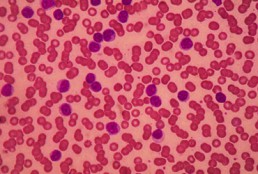
A 79-Year-Old Man With Relapsed Chronic Lymphocytic Leukemia
A 79-Year-Old Man With Relapsed Chronic Lymphocytic Leukemia
Age, Recent Treatment, Appear to Influence Severity of COVID-19 in Patients With CLL
Age, Recent Treatment Appear to Influence Severity of COVID-19 in Patients With CLL
Long-Term Results of Ibrutinib/Umbralisib Show Efficacy in CLL and MCL
Long-Term Results of Ibrutinib/Umbralisib Show Efficacy in CLL and MCL
This article was originally published by Targeted Oncology
Matthew S. Davids, MD, associate director of the Center for Chronic Lymphocytic Leukemia, director, Clinical Research for the Lymphoma Program at the Dana-Farber Cancer Institute, and associate professor of Medicine at Harvard Medical School, discusses the long-term follow-up of a phase 1/1b trial (NCT02268851) for patients with relapsed/refractory chronic lymphocytic leukemia (CLL) or mantle cell lymphoma (MCL) receiving ibrutinib (Imbruvica) and umbralisib.
The initial results were presented early in 2019 with about 2 years of follow-up, showing high rates of response in patients with CLL and MCL, according to Davids. There was good tolerability observed for these patients, and the investigators were able to identify the recommended phase 2 dose for umbralisib of 800 mg combined with the standard dose of ibrutinib.
The challenge with the initial report was that the follow-up for these patients was short, Davids says. The goal of the update at the 2020 European Hematology Association Congress was to present about 4 years of follow-up of the progression-free survival (PFS) and overall survival (OS) of the high-risk patients. The investigators also looked at the rates of complete remission, which increased over time.
For patients with MCL, the median PFS was around 11 months, and the median OS was about 2 and a half years. Davids thinks that this didn’t look much different than ibrutinib monotherapy, and it is hard to tell if there is a difference between monotherapy and this combination.
Davids says the investigators saw the bigger difference in the patients with CLL compared to historical control studies. There was about an 80% 4-year PFS in the high-risk CLL population and a 4-year OS of 90%. There are still many patients on the ibrutinib and umbralisib combination. The data set highlights the efficacy and safety of dual B-cell receptor blockade and warrants further study, he believes.

CLL Advocates NZ Newsletter Issue 1
CLL Advocates NZ Newsletter Issue 1
Welcome to our first CLL Advocates newsletter. Like many organisations, we weren’t able to accomplish very much over the lockdown period. We did, however, manage a Trustees’ teleconference to shape up our strategy for the next 12 months. One of the proposals made at that meeting was a monthly newsletter, so here is the first edition.
A huge number of lay and medical articles have been written about the COVID pandemic, and, as you may have seen on our website, we’ve published a number relevant to people living with CLL. See them here. One of particular interest was a consensus statement by Australasian haematologists on management of blood cancers in the COVID pandemic (published in May’s Internal Medicine Journal). It noted that, with a mean age of diagnosis of about 70 years, CLL patients are already likely to be in a high-risk group simply because of age. Advice specifically directed to CLL patients was:
- to delay planned therapy where possible
- to consider using oral agents over IV medications so as to avoid exposure to higher risk environments such as hospital chemotherapy units, for treatment of both initial therapy, and for relapsed/refractory disease (see our recent letter to Pharmac on this matter).
New Zealand has done extraordinarily well at this stage to contain the virus, though it should be noted that vaccination, if successfully developed, may present further challenges for CLL patients.
The CLLANZ Trustees’ meeting agreed that information/education initiatives on CLL should be high on our priority list. In this regard, a review of the current management of CLL by Dr Gillian Corbett, haematologist and trustee, has been published on our website. A detailed CLL patient information booklet is also now close to sign-off and will be published shortly.
In October this year we will be staging a half day or evening combined meeting/seminar on CLL in NZ with the Leukaemia & Blood Cancer (LBC) group, with leading NZ CLL specialists. This will be ‘in person’ in Auckland and also online on Zoom so that people from around the country can join in the discussion and if desired put questions to the speakers. Details will follow soon.
To ensure we reach as many people as possible who have an interest in CLL, we encourage you to become a ‘friend’ of CLL Advocates NZ – by signing up to our newsletter here and/or joining our private Facebook group. You can apply to join the group here.
More details of anticipated activities will follow in subsequent newsletters.
Meanwhile, now that we have passed the winter solstice, and are becoming adjusted to the new ‘normal’, stay well, physically, mentally and spiritually. And please remember that as well as our advocacy role, we want to be a source of knowledge and support for New Zealanders living with CLL, and their families and supporters. To help us achieve this we would welcome and appreciate your feedback, and your thoughts on how we can best achieve our mission.
With best wishes
Neil Graham FRACP, FRCP
Executive Director
CLL Advocates NZ

Three-Drug Combo Promising Against High-Risk CLL
Three-Drug Combo Promising Against High-Risk CLL
For patients with high-risk chronic lymphocytic leukemia (CLL), first-line therapy with a triple combination of targeted agents showed encouraging response rates in the phase 2 CLL2-GIVe trial.
Among 41 patients with untreated CLL bearing deleterious TP53 mutations and/or the 17p chromosomal deletion who received the GIVe regimen consisting of obinutuzumab (Gazyva), ibrutinib (Imbruvica), and venetoclax (Venclexta), the complete response rate at final restaging was 58. 5%, and 33 patients with a confirmed response were negative for minimal residual disease after a median follow-up of 18
Chemotherapy-Free Regimen Consisting of 3 Novel Agents for Previously Untreated, Poor Prognosis CLL
Chemotherapy-Free Regimen Consisting of 3 Novel Agents for Previously Untreated, Poor Prognosis CLL
Nearly 60% of evaluable patients with previously untreated, chronic lymphocytic leukemia (CLL) characterized by chromosomal deletion of 17p (del[17p]) and/or a deleterious TP53 mutation treated with obinutuzumab, ibrutinib, and venetoclax triplet therapy achieved either complete remission (CR) or a CR with incomplete recovery of the bone marrow, according to results of a single-arm, phase 2 study presented during the Virtual Edition of the 25th European Hematology Association (EHA) Annual Congress.
While less than 10% of patients diagnosed with CLL have disease characterized by del(17p), this biomarker is present in up to half of patients with refractory disease.2 Hence, there is an unmet need for efficacious and safe treatment regimens for this subgroup of patients. Furthermore, compounding this need is the finding that TP53 mutations, another biomarker of poor prognosis, have been reported to be present in approximately 90% of patients with disease characterized by del(17p) although only about 40% of those with TP53-mutant CLL also have del(17p).An unmutated IGHV gene is another risk factor for poor prognosis in the setting of CLL.2

Dr. Flinn on the Role of BTK Inhibitors in CLL
Dr. Flinn on the Role of BTK Inhibitors in CLL
This story was originally published on OneLive
Ian W. Flinn, MD, PhD, discusses the role of BTK inhibitors in chronic lymphocytic leukemia.
Ian W. Flinn, MD, PhD, director of the Blood Cancer Research Program, Sarah Cannon Research Institute, discusses the role of BTK inhibitors in chronic lymphocytic leukemia (CLL).
BTK inhibitors such as ibrutinib (Imbruvica), acalabrutinib (Calquence), and zanubrutinib (Brukinsa) have been transformative in the treatment of patients with B-cell malignancies such as CLL, mantle cell lymphoma, marginal zone lymphoma, and Waldenström’s macroglobulinemia, says Flinn.
In CLL specifically, BTK inhibitors have become a prominent frontline standard of care, adds Flinn.
Though, it is important to acknowledge that the toxicities that are associated with ibrutinib, including arthralgias, atrial fibrillation, and, though rare, significant bleeding, often lead to treatment discontinuation in patients with CLL.
'CLL flares’ reported after stopping ibrutinib
'CLL flares’ reported after stopping ibrutinib
Patients with ibrutinib-resistant CLL should remain on the BTK inhibitor until immediately before starting their next therapy, Australian haematologists have advised. In a Commentary article in Leukemia & Lymphoma, Dr Chloe Tang and Associate Professor Constantine Tam wrote that ‘CLL flares’ – accelerated CLL progression after ceasing ibrutinib – can be difficult to distinguish from …
Durable disease control achieved with BTKi salvage therapy in patients with CLL
Durable disease control achieved with BTKi salvage therapy in patients with CLL
Patients with chronic lymphocytic leukaemia (CLL) who progress on venetoclax can achieve durable disease control with Bruton tyrosine kinase inhibitor (BTKi) salvage therapy, new Australian research reveals. The study included 23 patients with refractory/relapsed CLL who received a BTKi (ibrutinib [n=21], zanubrutinib [n=2]) after ceasing the BCL2 inhibitor venetoclax due to progressive disease. After initiating …
To continue reading click here.